What’s in a name?
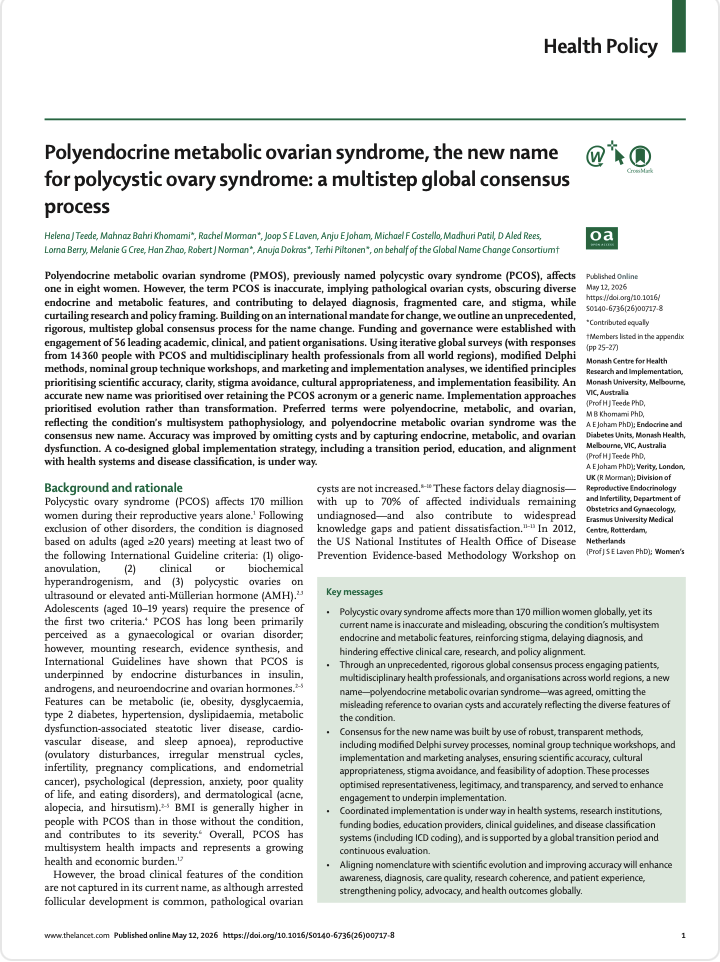
Polycystic Ovary Syndrome (PCOS) affects around one in eight women worldwide, yet its name has long been considered confusing and misleading. A recent global consensus has introduced a new term: Polyendocrine Metabolic Ovarian Syndrome (PMOS) – a change designed to better reflect the true nature of this complex condition.
This shift is more than just a rebrand. It represents a growing understanding that what was previously called PCOS is not simply an ovarian issue but a condition affecting multiple systems in the body. For individuals managing symptoms – and for dietitians supporting them – this new name signals an important evolution in both awareness and care.
Why PCOS needed a new name
The term “polycystic ovary syndrome” has been criticised because it places focus on “cysts” that are not actually the defining feature of the condition. In fact, many people diagnosed with PCOS do not have ovarian cysts, and the name can lead to misunderstanding among patients, clinicians, and the wider community.
More importantly, the name fails to capture the condition’s full scope. PCOS involves a complex interplay of hormonal imbalances, metabolic dysfunction, and reproductive challenges. Symptoms can include irregular menstrual cycles, fertility issues, excess androgen levels (which can affect skin and hair), and a higher risk of conditions such as type 2 diabetes, cardiovascular disease, and fatty liver disease.
This narrow focus has historically contributed to delayed diagnosis – up to 70% of cases remain undiagnosed – and fragmented care. It can also reinforce stigma, particularly in relation to fertility, which may not be the primary concern for many individuals.

What PMOS tells us about the condition
The new name, Polyendocrine Metabolic Ovarian Syndrome, reflects three key aspects of the condition:
- Polyendocrine highlights the involvement of multiple hormone systems, not just the ovaries
- Metabolic emphasises the role of insulin resistance, weight regulation, and cardiometabolic risk
- Ovarian retains the important reproductive component without overemphasising “cysts”
This terminology aligns with current evidence showing that insulin resistance is present in the majority of individuals with the condition and plays a key role in driving symptoms.
By acknowledging the metabolic component, PMOS also reinforces that this is a whole-body condition requiring a holistic management approach – well beyond reproductive health alone.

The Role of nutrition in managing PMOS
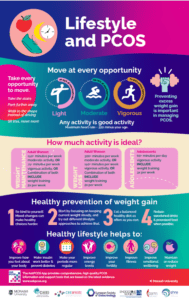
For dietitians, the inclusion of “metabolic” is particularly significant. Nutrition and lifestyle are central to managing PMOS, especially in addressing insulin resistance, inflammation, and weight-related symptoms.
Evidence shows that insulin resistance can amplify hormonal imbalances, contributing to symptoms such as irregular cycles and androgen excess. This means dietary strategies that support blood glucose regulation – such as balanced meals, adequate protein, fibre intake, and mindful (low glycemic index) carbohydrate choices—can have a meaningful impact.
Weight management, where appropriate, can also improve symptoms and reduce long-term health risks. However, it’s important to recognise that PMOS affects individuals across all body sizes, and care should always be personalised, realistic, and non-stigmatising.
A dietitian plays a key role in helping clients navigate this complexity – supporting sustainable habits, improving metabolic health, and ultimately enhancing quality of life.
What this means for women moving forward
During the transition period, both PCOS and PMOS will be used interchangeably, with a global rollout planned across healthcare systems, research, and education.
For clients, the new name may help validate their experience by recognising that their symptoms are not limited to reproductive health. It also supports more accurate diagnosis, clearer communication, and improved long-term management.
Ultimately, the move to PMOS is about improving understanding and outcomes. With better awareness of the metabolic and hormonal drivers of the condition, individuals can access more targeted support—including effective nutrition strategies that address the root causes, not just the symptoms.
Dietitians are trained to take a key role in assisting women with PMOS to manage their symptoms. Here at Lifestyle Maternity, specialist women’s health dietitians are able to tailor a program to support you to adapt guideline recommendations to your lifestyle and preferences. We look forward to supporting you on your journey to better health and quality of life. For further information book an appointment with a Lifestyle Maternity Dietitian or enrol in an online, self-paced course.










 Find us on
Find us on